
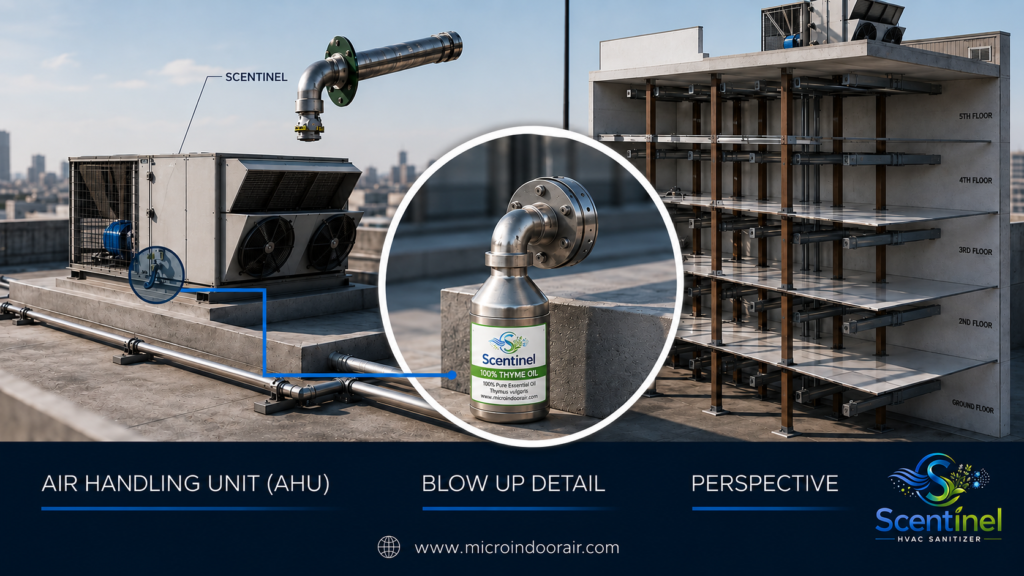
Transform indoor air into a strategic asset with InMicro – Scentinel®, a US-patented HVAC diffuser system that delivers continuous 24/7 indoor environmental support using botanical countermeasure technology.
Improve indoor environmental quality while supporting healthier spaces and stronger operational performance across facilities.
✓ Passive 24/7 Operation
✓ No Moving Parts, No Electronics, No Maintenance Burden
✓ US-Patented HVAC Diffuser Technology
✓ Healthcare, Commercial, Hospitality & Industrial Applications
Cleaner Air. Simplified.
Why InMicro – Scentinel ®
PASSIVE PROTECTION. CONTINUOUS PERFORMANCE
Unlike traditional air treatment systems, InMicro Scentinel® integrates directly into HVAC systems as a passive diffuser, requiring no power, no fans, and no mechanical components.
Traditional systems rely on filtration, airflow, and mechanical maintenance.
InMicro Scentinel® delivers a continuous environmental countermeasure at the air distribution level.

Key Advantages:
- No moving parts
- No electrical components
- Silent operation
- Minimal maintenance requirements
- Continuous 24/7 deployment
- Facility-wide HVAC integration
Traditional Air Treatment vs. Scentinel®
| Traditional Systems | Scentinel® |
|---|---|
| Requires power-intensive equipment | Passive operation |
| Moving parts subject to wear | No moving parts |
| Fans and motors require maintenance | Minimal maintenance |
| Limited operation zones | Continuous coverage |
| Frequent service intervals | Long-lasting deployment |
| Mechanical approach | Botanical countermeasure technology |
Our Efficacy Testing Method:
ATP (Adenosine Triphosphate)
ATP Detection is the only method that directly assesses living cells from any type of microbe, providing an immediate indication of microbial contamination in your sample.
How Hospitals Detect Viruses Today
Hospitals today are using a fast and reliable method called ATP testing to check if harmful germs are present on surfaces. ATP (Adenosine Triphosphate) is found in all living things — including viruses and bacteria. By testing for ATP, hospitals can quickly see if an area is truly clean or if dangerous microbes are still there.
The big advantage of ATP testing is speed. Results are available in 10seconds, which means cleaning staff and infection control teams can act right away to protect patients, visitors, and staff. With threats like COVID-19 and other infections, hospitals rely on this method as a frontline tool to keep environments safe and healthy.

PROVEN RESULTS
Real-World Healthcare Outcomes
A 112-bed healthcare facility implementing continuous botanical countermeasure delivery observed measurable improvements in environmental and prescribing outcomes.
| Outcome | Result |
|---|
| Airborne Contamination | ↓ 90% |
| Antibiotic Prescriptions | ↓ 70% |
| Corticosteroid Prescriptions | ↓ 67% |
| Mucolytic & Bronchodilator Use | ↓ 100% |
FEATURED INSIGHT
Protecting Healthcare Operating Margins
Protecting Healthcare Operating Margins
Improving indoor air quality can contribute not only to healthier environments but also to stronger healthcare economics and operational efficiency.

INDUSTRY APPLICATIONS
Healthcare
Improve indoor environmental quality and occupant comfort.
Hospitality
Enhance guest wellness and environmental experience.
Industrial Facilities
Support workforce health and indoor air quality management
CASE STUDIES
Healthcare Facility Deployment in Italy | 2016
Documented reductions in airborne contamination and improved operational outcomes.
Conducted in a 112-bed residential healthcare facility in Italy over 5 months. One section of the facility received standard cleaning plus essential oil diffusion, while another section received standard cleaning alone.
Essential oils were dispersed using ultrasonic vaporizers operating 16 hours per day. Microbial contamination was measured monthly from tables, cabinets, and handrails using contact slides.
Smile Dental Implant Centre in Surrey British Columbia | May 2020
In May 2020, InMicro Indoor Air Inc. conducted an environmental surface and air assessment following the installation of Scentinel® commercial HVAC diffusers at the Smile Dental Implant Centre in Surrey, BC.
The objective was to observe changes in environmental microbial load (bacteria, virus, and mold indicators) following continuous exposure to a botanical vapor-based indoor air treatment.
Swab samples were collected prior to installation and again after 48 hours of continuous Scentinel® operation and analyzed by an independent commercial laboratory in Richmond, BC for total bacterial colony forming units (CFUs).
Ready to Improve Indoor Air Quality?
Discover how InMicro – Scentinel®, the US-patented HVAC diffuser system, can help create healthier indoor environments and support stronger operational outcomes.
Blog
Why Do ATP Readings Drop After Thyme Oil Vapor Treatment in Operating Rooms — Even Without Cleaning?
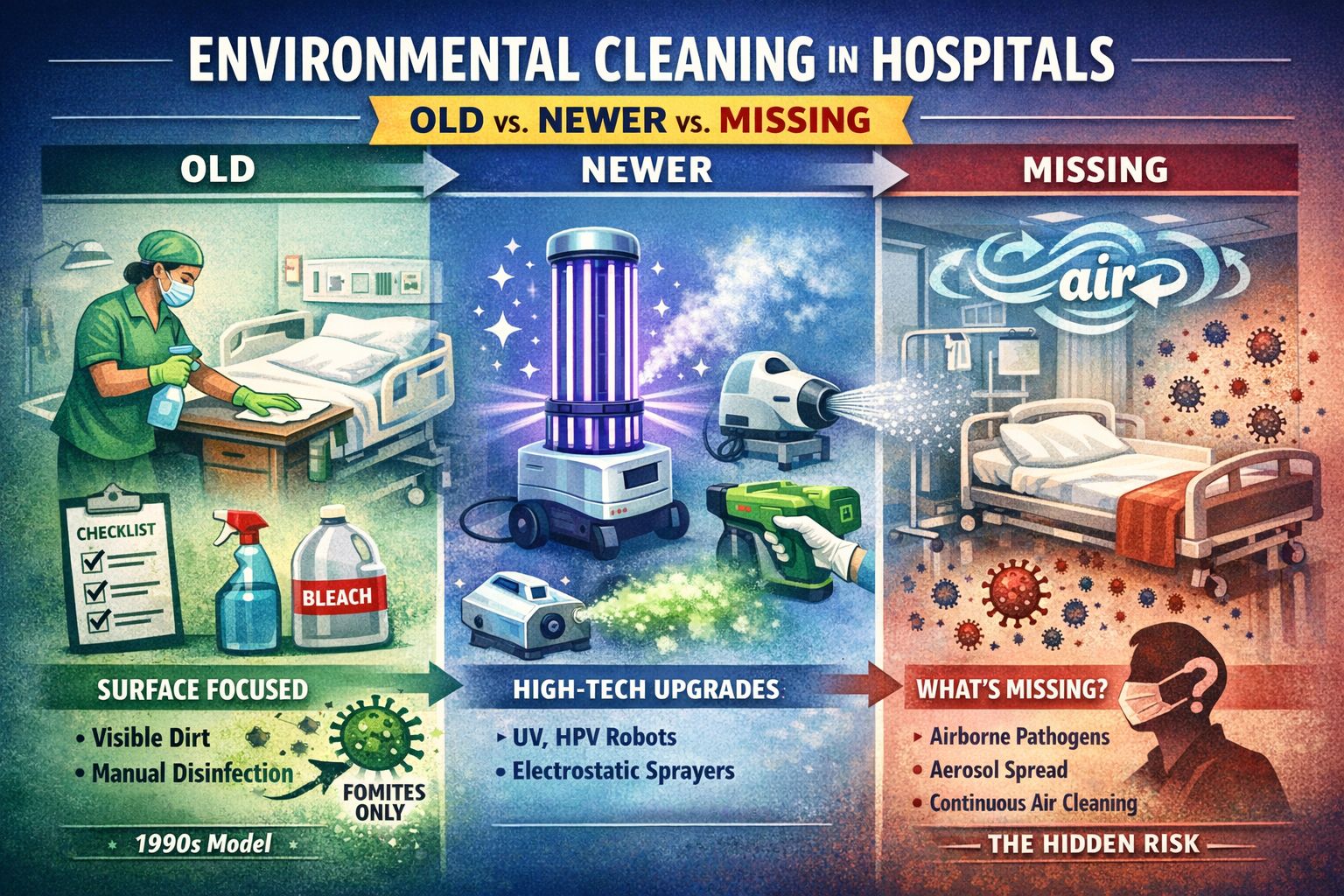
What “environmental cleaning” means (hospital context)
Vapour Technology for Infection Control

Infection Prevention and the Role of Fractional Aerosol Filtration Efficiency in In-duct Ventilation Air Cleaners.

Preventing Infections in the Built Environment: The Need for Air Sanitizers with Essential Oil Vapors




































